
A 38-year-old patient in Phoenix is considering gastric sleeve. She has been thinking about it for nearly two years. Her insurance does not cover bariatric surgery. Out-of-pocket in Arizona can start around 22,000 dollars. Tijuana suddenly feels less like a discount option and more like the first place where surgery becomes financially possible. A friend from work flew to Tijuana in 2024 and came back with a story that made the option feel real. The friend told her the surgeon's name on a Saturday afternoon.
By the time that patient submits a form on a Tijuana clinic site, she has watched three YouTube videos of surgeons explaining the difference between sleeve and bypass. She has read a Reddit thread comparing four clinics. She has asked ChatGPT what BMI she needs. She has asked Gemini whether revision surgery in Mexico is safe. She has scrolled through twenty reviews. She has cross-referenced two surgeons on Doctoralia and one on RealSelf. She has texted her friend to ask if anyone she knew had complications.
The clinic sees a lead. The patient sees the end of a research process that started months ago.
The problem with most bariatric SEO is not that it ignores Google. It is that it treats the Google click as the beginning of the decision.
The 30-second summary
SEO for bariatric surgeons still matters. Rankings and clicks are useful. They are also incomplete. Bariatric patients now research across Google, ChatGPT, Gemini, Perplexity, Claude, Google AI Overviews, Reddit, YouTube, reviews, directories, and private referrals before any form is submitted. The new goal for a bariatric practice is not just to rank. It is to be findable, extractable, verifiable, and persuasive across the surfaces where the patient is actually making her decision.
This is where SEO, GEO (generative engine optimization), AEO (answer engine optimization), and zero-click marketing overlap. Traditional SEO helps the patient find you. AI visibility helps the patient understand, compare, and trust you before she contacts the practice. Both matter. The bariatric practices that figure out the second piece in 2026 will be better positioned to reduce wasted acquisition spend and improve consultation quality than the ones that keep optimizing only for the click.
SEO still matters. It is just not the whole system.
Bariatric surgeon SEO still matters. Technical SEO, page speed, title tags, schema markup, internal linking, local SEO, Google Business Profile optimization, procedure pages, indexability, and crawlability all still matter. If your gastric sleeve page is not indexed, no one is going to find it from search. If your Google Business Profile has wrong hours and a missing service list, the local pack will not surface you. None of that has changed.
What has changed is that SEO is no longer the entire system. SEO is the foundation layer. On top of that foundation, a modern bariatric practice now needs to think about AI visibility, trust-building infrastructure, source extraction logic, and the quality of patient decisions before any click registers.
Rankings can help the patient find you. They do not automatically help the patient trust you.
A bariatric surgeon ranking position one for "gastric sleeve Tijuana" might still lose the patient to a competitor ranking position three. Why? Because the competitor's reviews mention the procedure by name. Because the competitor's doctor bio explains why a US patient would trust him specifically. Because when the patient asked ChatGPT about safety, the competitor's name appeared in the answer. Because the competitor's pricing page made the package transparent enough that the patient stopped researching alternatives.
Ranking is necessary. It is not sufficient.
The full operator-side argument for this shift is in zero-click marketing for medical tourism, which goes deeper into the measurement gap.
What bariatric patients ask before they contact you
Bariatric patients do not search "bariatric surgeon near me" and book the first result. The decision is too high-stakes, too expensive in cash terms, and too irreversible.
These are real prompts and queries we see bariatric patients running before contacting a practice. Some on Google. Some on ChatGPT or Gemini. Some on Reddit. Some on YouTube. All before the form:
- Is gastric sleeve safer in Mexico?
- How much does gastric sleeve cost in Tijuana?
- Gastric sleeve vs gastric bypass, which is better for me?
- What BMI do I need for bariatric surgery?
- Who is the best bariatric surgeon in Tijuana?
- Is the surgeon board-certified in Mexico?
- What happens if I have complications after returning to the US?
- How many days do I need to stay in Tijuana?
- What is included in the bariatric package?
- Can I finance bariatric surgery in Mexico?
- What do real patients say about recovery?
- Is revision bariatric surgery riskier?
- Can I convert a lap band to sleeve or bypass?
- How long before I can fly home after gastric sleeve?
- What labs and medical tests are required before surgery?
- What kind of follow-up do I get after returning home?
- What if I cannot lose enough pre-surgery?
- Is the hospital accredited?
Each of these questions has a specific answer space. The patient is not asking "is bariatric surgery good." She is comparing options against her own situation. She is checking your answers against three other clinics. She is forming a position before she contacts you.
If your site, your reviews, your external profiles, and the AI systems that summarize all of them cannot give clear answers to most of these questions, the patient will either contact a competitor first or arrive at your consultation still skeptical. Both outcomes raise your cost per booked surgery, even if your ranking stays the same.
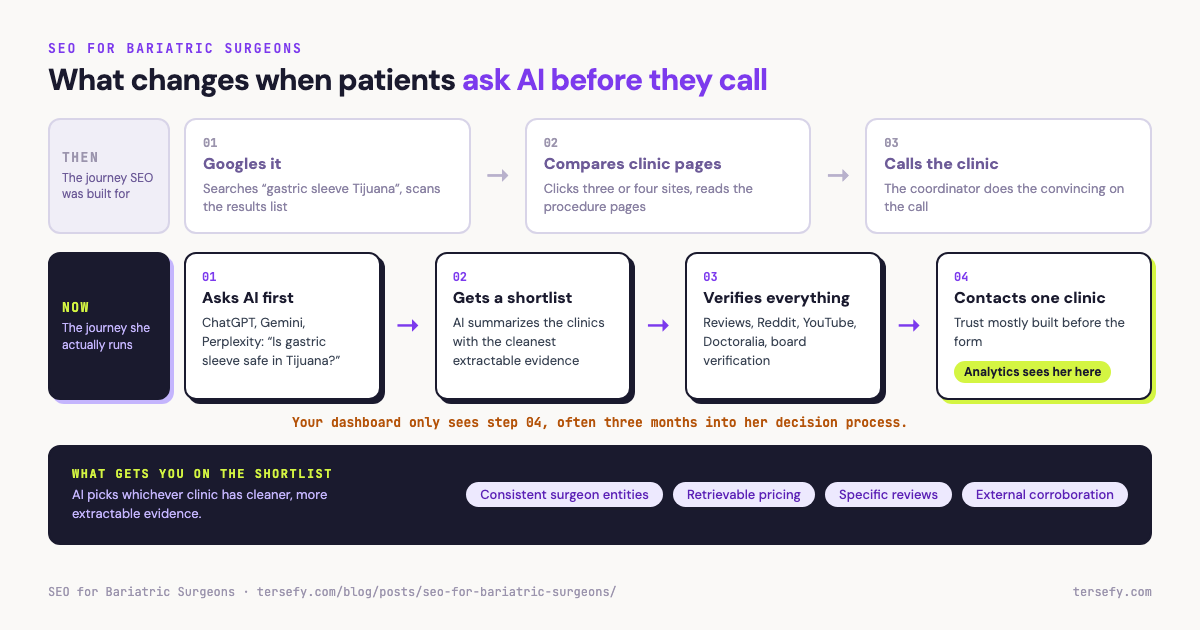
The bariatric patient decision journey
Seven stages, often months long. Each card shows the question the patient is asking, where she is asking it, the evidence she needs, and the measurement gap your analytics never records. Your dashboard only sees stage six.
The old bariatric SEO checklist is incomplete
For about fifteen years, bariatric SEO has looked roughly the same. The standard checklist:
- Keyword-targeted pages for gastric sleeve, gastric bypass, and revision surgery
- Title tag optimization with primary keyword and location
- Local SEO with consistent NAP across directories
- Google Business Profile with photos, hours, services, and review responses
- Backlink building from medical directories and PR placements
- Blog posts on weight-loss topics
- Before-and-after photo galleries
- Patient review collection
- Basic LocalBusiness or Physician schema
This checklist is not wrong. It is incomplete.
It can get your gastric sleeve page indexed. It cannot make your surgeon understandable to a system that summarizes content for a patient who never visits your site.
It can rank for "gastric sleeve Tijuana." It cannot explain why a patient should trust your specific doctor over the four other clinics ranking on the same page.
It can bring leads. It cannot improve the quality of the consultations once those leads enter your sales process.
It can hide pricing behind a form and force the patient to ask. In 2026, that often costs you the lead entirely, because the patient already asked ChatGPT for a price range and got an answer that came from a competitor's transparent pricing page.
It can ignore what AI systems extract from your public sources. That is the largest blind spot. If your site, your doctor bios, your reviews, and your external profiles are inconsistent or thin, an AI assistant asked "best bariatric surgeon in Tijuana for revision" will pick whichever clinic has cleaner, more extractable evidence. The patient never sees your name in the answer.
Old SEO vs AI visibility: what gets added
AI visibility is not a replacement for SEO. It is a second layer added on top. Both columns are still valid in 2026. If you have most of the left and almost none of the right, you have an SEO program. If you have both, you have a modern bariatric visibility program.
- Keyword targeting and rankings
- Organic traffic volume
- Google Business Profile completeness
- Backlink portfolio
- Generic blog content
- Contact form as primary conversion
- Doctor entity clarity across the open web
- Procedure-to-doctor mapping in structured data and prose
- FAQs written in a format AI systems can extract
- Pricing context that is retrievable without filling a form
- Review specificity with procedure, surgeon, city, recovery, and outcome named
- External source alignment across directories, hospital pages, interviews, profiles
- Prompt tracking across ChatGPT, Gemini, Perplexity, Claude, and Google AI Overviews
- AI answer testing for your top patient questions
- Source corroboration so claims on your site are backed by external evidence
- Conversion quality measurement after the form, not just lead volume
The new SEO checklist for bariatric surgeons
This is what a practical, modern bariatric SEO program looks like in 2026. It includes everything from the old checklist plus the AI visibility layer that was missing.
Clear doctor entity pages
Each surgeon in your practice needs a dedicated page that includes full name, credentials, training, specialty board certification, years in practice, procedures performed, hospital affiliations, and a current photo. The page should be linked from every procedure page that surgeon performs. The information on the page should match what appears on the surgeon's external profiles on Doctoralia, RealSelf, hospital directories, and board verification sites. Inconsistency between your site and external sources is one of the largest reasons AI systems fail to confidently identify a surgeon.
Procedure-specific pages for every surgery you actually perform
A single page titled "Bariatric Surgery" is not enough. You need separate, substantial pages for gastric sleeve, gastric bypass (Roux-en-Y), mini gastric bypass (one-anastomosis), revision surgery, lap band conversion to sleeve or bypass, and any other procedure your practice offers. Each page should explain candidacy, the procedure itself, recovery timeline, expected outcomes, and risks. Generic content reused across procedures hurts both your SEO and your ability to be extracted accurately by AI systems for procedure-specific patient questions. For the page type that matters most, see our gastric sleeve procedure page guide.
Physician schema and procedure schema
Use Physician schema for each surgeon with full credential data, board certifications, and worksFor relationships pointing to your clinic organization. Use MedicalProcedure or relevant medical schema on each procedure page when accurate and not misleading. Schema is not magic. It is structured data that helps both Google and AI systems extract clean facts from your site rather than guessing from prose. The full primer on entity-level work for surgeons is in AI visibility for Tijuana surgeons.
FAQs written around real patient questions
The patient question list from earlier in this article is your FAQ source list. Each procedure page should have a FAQ section that answers the questions patients actually ask, in plain language, with one direct answer per question. Avoid marketing copy. Avoid hedging. Answer the question, then expand. FAQs in this format are the most extractable content type for AI assistants and Google AI Overviews.
Transparent package context and starting price ranges
The argument for hiding pricing was that it forces the patient to contact you so a coordinator can sell. In a zero-click world, hiding pricing forces the patient to ask ChatGPT, which will return whatever public price ranges it can find from your competitors. Publishing a starting price range with package inclusions, exclusions, and financing context lets you control the narrative the patient brings into the consultation. The longer argument for this is in AI pricing transparency for Tijuana medical tourism.
Review strategy that encourages specificity
A five-star review that says "great service" tells the next patient nothing. A four-star review that says "Dr. Lopez did my gastric sleeve in March, recovery was three days, I lost 75 pounds in eight months, follow-up calls came as scheduled" is worth fifty generic five-star reviews. Train your coordinators to ask reviewing patients to mention procedure name, surgeon name, city, recovery timeline, and outcome. Specificity is what AI systems extract. Generic praise gets averaged into noise. More on this in our bariatric surgeon reviews deep dive.
External source alignment
Your surgeon's name and credentials should appear consistently across Doctoralia, RealSelf, ISAPS or relevant board listings, hospital affiliation pages, conference speaker bios, interview features, and any directory that medical tourism patients actually use. Inconsistency between sources signals low confidence to AI systems. Cleaning up external profiles is often higher leverage than writing more blog posts.
Internal linking from doctor to procedure and back
Each surgeon page should link to every procedure that surgeon performs. Each procedure page should link to the surgeons who perform it. Each pricing context should link to the procedure it describes. Each safety section should link to the relevant procedure page. This linking pattern helps Google understand the relationship between surgeon, procedure, and outcome. It also helps AI systems retrieve consistent answers when a patient asks about a specific doctor performing a specific procedure.
Prompt tracking as a measurement layer
Pick fifteen to thirty prompts your patients actually ask. Run them across ChatGPT, Gemini, Perplexity, Claude, and Google AI Overviews on a recurring schedule. Track whether your clinic and surgeons appear in the answers, in what context, and against which competitors. This is not a vanity metric. It is the closest available proxy for AI visibility, the same way keyword rank tracking became the proxy for SEO a decade ago. The full workflow is in our ChatGPT prompt tracking deep dive.
Conversion tracking after the patient contacts the practice
Most bariatric practices measure leads. Fewer measure consultation booking rate. Fewer still measure surgery booking rate. Almost none measure the time from first patient contact to surgery, the channel each booked patient said they came from, or the reason patients dropped out. Lead volume without downstream tracking can hide a lot of waste.
Self-reported attribution at the consultation stage
The simplest, most underused measurement tool in bariatric marketing is asking the patient: "Before you contacted us, what made you decide we were worth considering?" Coordinators should ask this in every consultation. The answers reveal what the patient actually saw, which is almost never what your analytics shows.
Post-quote follow-up measurement
After a quote is sent, what percentage of patients book? What percentage go silent? Of the silent ones, how many booked elsewhere? How many delayed indefinitely? Most practices have no idea. The post-quote silence is where most bariatric revenue is lost, and almost none of it is visible in SEO dashboards.
Where bariatric SEO usually fails
The pattern of failures is consistent across bariatric practices. They are not exotic. They are predictable and most of them are cheaper to fix than to leave broken.
Thin doctor bios and generic procedure pages
The most common failure is a 200-word doctor bio that says "Dr. Smith is a board-certified surgeon with 20 years of experience" and a procedure page that reads like a Wikipedia summary. AI systems extracting from these pages get almost nothing they can use. The patient comparing your surgeon to three others sees no reason to pick yours. Thin content fails twice: it does not help SEO ranking against substantive competitors, and it does not give an AI assistant enough material to identify or explain the surgeon.
A related variation: the same generic content reused across multiple doctors in the same practice. If three of your surgeons share a 200-word bio with only the name changed, AI systems have no way to distinguish them. The "best gastric sleeve surgeon in Tijuana" prompt has no extractable basis for picking any one of them over the other two.
No clear surgeon-to-procedure mapping
Many practices have doctor pages and procedure pages but no clear connection between them. The patient asking "who at this clinic does revision surgery" has to guess. The AI assistant trying to answer the same question has to guess too. Both will guess wrong sometimes, and the wrong guess is not always in your favor.
Hidden pricing with no package explanation
Pricing that lives entirely behind a form forces the patient to ask elsewhere first. In 2026, elsewhere is increasingly an AI assistant that has already extracted price ranges from competitor sites. By the time the patient contacts you, she has a number in her head, and it did not come from you. If she contacted three clinics for quotes and yours arrives last, she has already anchored her expectation.
Reviews without procedure or surgeon specificity
A wall of five-star reviews that all say "amazing experience" gives the AI assistant nothing to extract. It also gives the next patient nothing to anchor against. Reviews are one of the highest-leverage trust signals in bariatric, and they are often the most generic content on the site.
Weak external corroboration
If your surgeon's credentials live only on your website, AI systems have one source. If they appear consistently on Doctoralia, RealSelf, hospital pages, board verification, and interview features, AI systems have five corroborating sources. The single-source problem is invisible until you ask an AI assistant about your surgeon and watch what it returns.
No safety, aftercare, or travel content
Bariatric patients flying to Tijuana have specific concerns: complication management after returning to the US, how many days to stay, when they can fly, what labs to do at home, how follow-up works across borders. Most bariatric sites have nothing on any of these. The patient who cannot find answers on your site finds them on a competitor's site, or on Reddit, where the competitor's name appears more often than yours.
No differentiation between procedure intents
The patient researching revision surgery is not the same patient researching first-time gastric sleeve. The patient researching mini-bypass is not researching Roux-en-Y. Treating these as one funnel costs you the patients searching the more specific intents, which often have higher commercial value and less competition.
No measurement of AI answers
Most bariatric practices have never seen what ChatGPT, Gemini, or Google AI Overviews say about them. They are optimizing for a layer of search they cannot see. That is a structural disadvantage against any competitor that has started tracking.
What AI visibility changes for bariatric surgeons
AI does not just match keywords. It summarizes what it can retrieve and verify. The shift from match to summary is the whole story.
For a bariatric surgeon, this means AI systems need enough extractable evidence to understand who the doctor is, what procedures the doctor performs, where the surgery happens, what credentials matter, what the package includes, what safety standards exist, what real patients say, how the practice compares to alternatives, what happens before and after surgery, and why a US patient might trust this specific option.
When that evidence is strong, AI has more material to retrieve, compare, and explain when a patient asks. When the evidence is weak, inconsistent, or trapped inside ads and gated forms, AI has less to work with. The patient gets a thinner answer about your practice, or no mention at all, while a competitor with better evidence gets cited.
This is not about AI recommending your clinic. No one can promise that. It is about whether AI has enough information to even include you in the comparison the patient is building. If you are not in the comparison, you are not in the consideration set. If you are not in the consideration set, you do not get the form submission, no matter how well your gastric sleeve page is ranking in traditional search.
The bariatric practices that win in this environment are not the ones with the loudest marketing. They are the ones with the cleanest, most retrievable evidence.
What patients actually ask: a prompt map
Pick a procedure, a concern, and a location to see the prompts patients run before they contact anyone, the content that answers each one, and the page you would need to build. Each card is a gap in most clinic content libraries.
What Tersefy measures for bariatric practices
Tersefy does not only ask "do you rank?" It asks a different set of questions that map directly to how bariatric patients are deciding in 2026:
- Can AI find each surgeon in the practice by name?
- Can AI connect each surgeon to the specific procedures they perform: sleeve, bypass, mini-bypass, revision, band conversion?
- Can AI explain why a US patient would trust this practice specifically over alternatives?
- Can AI identify pricing context for the procedures the practice offers?
- Can AI cite sources beyond the clinic's own site to corroborate claims?
- Can the practice track which prompts mention them, which mention competitors, and which mention neither?
- Does the patient arrive at the form with trust already partially built, or still in active evaluation?
This is where SEO, GEO, AEO, and zero-click marketing overlap. They are not four separate disciplines competing for budget. They are layers of the same problem: helping the right patient find the right answer at the right stage of her decision.
Tersefy AI works before the form. It addresses the evidence layer that determines whether the patient arrives convinced, evaluating, or still skeptical. AI Closer System works after the form, on the post-contact bottleneck of response time, qualification, and conversion to consultation. Tersefy AI vs AI Closer System is a useful distinction, but the work that compounds over months is the work that happens before the patient ever fills out a form.
A worked example of this approach applied to a multi-surgeon practice is in our VIDA case study, which walks through how doctor entity work, procedure-page restructuring, review specificity, and prompt tracking moved together across the same twelve-month window.
Practical next steps
If you do nothing else this quarter, do these ten things. They are ordered roughly by impact-to-effort ratio for most bariatric practices.
- Audit each doctor page. Read it like a patient comparing four clinics. Does it tell you what makes this surgeon different? Does it match what is on Doctoralia, RealSelf, and hospital directories?
- Audit each procedure page. Sleeve, bypass, mini-bypass, revision, band conversion. Each should be a substantive page, not a paragraph inside a general bariatric page.
- Run your own prompts in AI systems. Ask ChatGPT, Gemini, Perplexity, Claude, and Google AI Overviews about gastric sleeve in Tijuana, revision surgery in Mexico, best bariatric surgeon in your city. See what comes back. Note who is mentioned and who is not.
- Check whether pricing context is extractable. Can an AI assistant cite a starting price range from your site, or only from competitors?
- Read your last 50 reviews. How many mention a specific procedure, surgeon, recovery timeline, or outcome? Reviews without specifics are noise.
- Align external profiles. Same credentials, same procedure list, same photo, same affiliations across every directory your patients actually use.
- Add internal links from doctor to procedure and back. The smallest, cheapest fix on this list. Often the most underdone.
- Track consultation quality, not only lead volume. What percentage of leads booked a consultation? What percentage of consultations booked surgery? Which channels actually produce booked surgeries?
- Ask every new patient: "What did you see about us before you reached out?" Write the answers down. After 30 patients, patterns appear that no analytics tool will show you.
- Build a prompt-tracking baseline. Pick 20 prompts. Run them monthly. Track changes. This is your AI visibility equivalent of keyword rank tracking.
None of these require a new agency contract. Most of them require an afternoon, a spreadsheet, and the willingness to look at what is actually happening.
If you want to see what AI says about your practice today
If you want to know whether AI can already find, name, and explain your bariatric practice, start with the Free AI Visibility Scorecard. It will tell you which surgeons in your practice are findable, which procedures are connected to them in AI answers, where external sources support your claims, and where the gaps are.
It will not promise that AI will surface your clinic tomorrow. No one can promise that. What it will tell you is whether the evidence layer your bariatric practice depends on is intact or missing.
Quick answers
What is SEO for bariatric surgeons?
SEO for bariatric surgeons is the practice of making a bariatric clinic's content, surgeon entities, and procedure pages findable and understandable by search engines. In 2026, that includes both traditional ranking work and the AI visibility layer that determines how AI assistants describe the practice to patients.
Why is traditional SEO no longer enough for bariatric practices?
Patients now research across AI assistants, Reddit, YouTube, and reviews before any click registers. Ranking position one for gastric sleeve in your city does not help if the AI summary the patient reads first mentions a competitor. SEO is still necessary, but the layer above SEO is where most decisions are now formed.
How does AI visibility affect bariatric patient acquisition?
AI visibility determines whether your surgeons and procedures appear in the answers patients read before contacting any clinic. Practices with extractable, consistent, corroborated evidence give AI systems more usable material to retrieve, compare, and explain. That can help patients reach the form with stronger trust already built.
Should bariatric surgeons publish pricing?
Publishing a starting price range with package context is often the stronger move, especially in cross-border markets where patients compare clinics before contacting anyone. If you do not publish a range, the patient asks ChatGPT, which returns whatever range it can find from competitors. You either control the narrative or someone else does.
What should a bariatric surgeon measure besides leads?
Consultation booking rate, surgery booking rate, time from first contact to surgery, self-reported attribution at consultation, post-quote follow-up outcomes, and prompt visibility across AI assistants. Lead volume alone hides too much for a long-cycle category like bariatric.
What pages should a bariatric surgeon's website include?
A dedicated page per surgeon, a substantive page per procedure (sleeve, bypass, mini-bypass, revision, band conversion), a transparent pricing page, a safety and aftercare page, a returning-home page for US patients, and FAQ blocks that answer real patient questions in extractable format.
How is GEO different from SEO for bariatric surgeons?
GEO does not replace SEO. It extends it. SEO makes your pages findable to search engines. GEO makes your evidence retrievable, verifiable, and explainable by AI assistants. A bariatric practice in 2026 needs both, working in the same direction.