
A US patient comparing gastric sleeve in Tijuana is not looking for the Wikipedia version of the procedure. She has read it three times. She wants to know if she qualifies at her BMI, what your package actually includes for the price you quote, who is going to perform the surgery, how safe the hospital is, how many days she has to stay, what happens if she has a leak after she gets home to Phoenix, and whether your clinic has handled patients like her before.
Most gastric sleeve pages answer the procedure. The better ones answer the decision.
That difference is the whole article.
The 30-second version
Gastric sleeve SEO is not only about ranking for "gastric sleeve." That game has been too crowded for years. The new game is whether your page can do three things at once: rank in traditional search, get extracted accurately by AI assistants, and walk a serious patient closer to a booking decision before she ever fills out a form.
A modern gastric sleeve page is not a keyword page. It is a decision-support asset. It connects the procedure to the surgeon, the package, the price context, the safety record, the recovery timeline, the reviews, and the aftercare protocol. This is where SEO, GEO (generative engine optimization), AEO (answer engine optimization), and consultation quality stop being separate disciplines and start being the same job.
The full system-level argument for why this matters is in our broader guide, SEO for bariatric surgeons. This article zooms into the most important page type in that system.
Why most gastric sleeve pages are too thin
Open three random gastric sleeve pages on Tijuana clinic sites. You will see the same pattern.
A generic definition of gastric sleeve, copied roughly from any patient education site. A vague reference to "experienced surgeons" without naming anyone. No BMI eligibility. No package explanation. A price that is either hidden behind a form or written as a range without context for what is or is not included. No mention of the actual hospital. A "recovery" section that says you will feel better in a few weeks. No travel logistics for someone flying from Phoenix or Dallas. No aftercare protocol. Reviews that say "amazing experience." Almost no internal links.
That page can rank. It can also fail every other thing you actually need it to do.
It cannot tell the patient who is going to perform her surgery. It cannot explain to an AI system why your surgeon should be cited when a patient asks "best bariatric surgeon in Tijuana." It cannot remove enough uncertainty for the patient to skip the next four clinic websites and fill out your form first. It cannot give your coordinator a stronger lead to work with on the consultation call.
A thin gastric sleeve page is not just bad SEO. It can be one reason your cost per booked surgery is higher than it needs to be.
What a gastric sleeve page needs to answer
The patient is not asking one question. She is running a list. Real prompts and queries we see bariatric patients running before they fill out any form:
- Am I a candidate for gastric sleeve at my BMI?
- What BMI do I need?
- How is sleeve different from bypass for someone in my situation?
- Who is going to perform the surgery?
- What credentials matter for a bariatric surgeon in Mexico?
- How much does gastric sleeve cost in Tijuana?
- What is included in the package and what is not?
- How many days do I need to stay in Tijuana?
- What labs and tests do I need before surgery?
- What happens if I have complications after I return home?
- How does follow-up work when the surgeon is in another country?
- What do real patients say about recovery and outcomes?
These are not just FAQ items to bolt onto the page. They are the conversion questions. Each one that goes unanswered on your page is either a patient who contacts a competitor first or a patient who arrives at your consultation still evaluating. Both options cost you money.
They are also the extraction points AI systems look for. The clearer your answers, the more material an AI assistant has to retrieve, compare, and explain when a patient asks. The vaguer your answers, the more an AI assistant has to guess. AI guesses are not always in your favor.
The ideal gastric sleeve page structure
This is the section order that actually works in 2026. It looks longer than what most practices currently publish. That is part of the point.
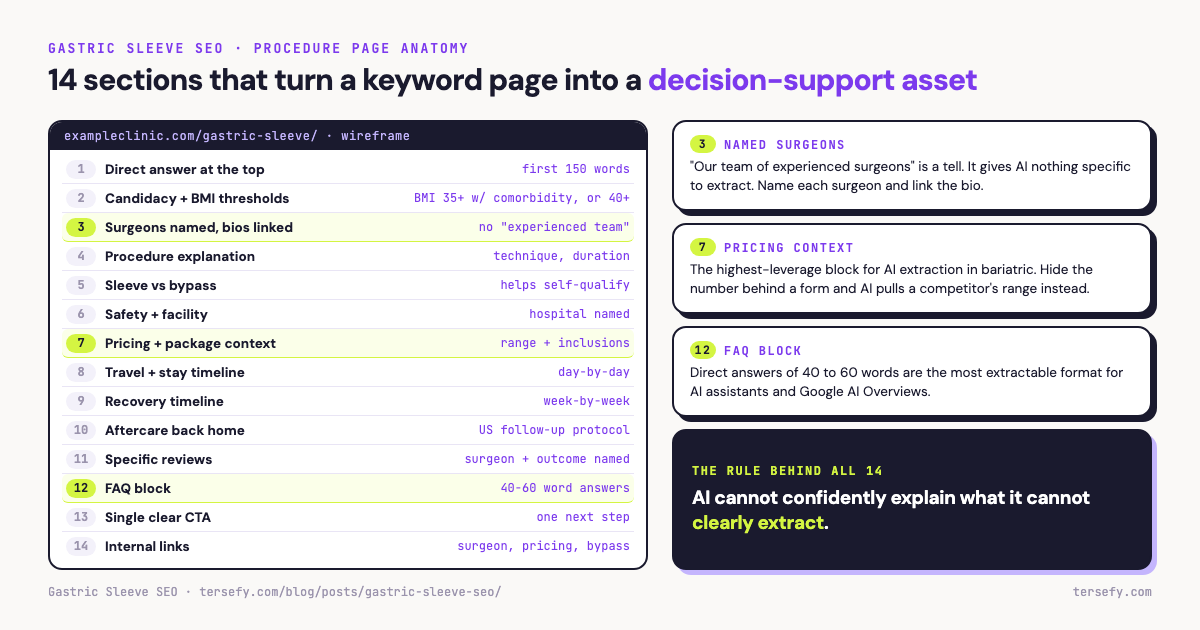
Direct answer at the top
The first 100 to 150 words should answer the core question in plain language. What is gastric sleeve, who is it for, what does it accomplish. Patient first, then SEO, then AI extraction. Most clinic pages bury this under hero images, contact forms, and welcome paragraphs. Move it to the top.
Who the procedure is for
Candidacy section. BMI thresholds and clinical criteria, often including BMI 35 or higher with comorbidities or BMI 40 or higher without, depending on the surgeon's evaluation and medical guidelines. Common comorbidities that qualify (type 2 diabetes, hypertension, sleep apnea, NAFLD). Patients who are typically not candidates (active substance abuse, certain psychiatric conditions, BMI under threshold without comorbidities). This section is where you stop wasting consultations on patients who were never candidates in the first place.
Surgeon connected to the procedure
The surgeons at your practice who perform gastric sleeve, by name, with a one-paragraph credibility summary on each and a link to their full bio. If three surgeons in your practice perform sleeve, list three. If only one does, list one. Do not write "our team of experienced surgeons." That phrase is a tell. It tells the AI system you have nothing specific to extract.
Procedure explanation
What actually happens during surgery. Laparoscopic technique, stomach reduction percentage, often described in patient education as roughly 75 to 85 percent, depending on technique and anatomy, surgery duration, anesthesia approach. This section should be written by or with the surgeon, not by a copywriter who has never been in an OR.
Sleeve vs bypass
A short comparison section helps the patient self-qualify and reduces consultation time wasted on basic procedure differences. Mention candidacy differences (severe reflux history typically points to bypass), weight loss expectations, reversibility, and recovery comparison. Link to your bypass page. Internal linking between procedure pages signals procedure-doctor mapping to both Google and AI systems.
Safety and facility
Hospital name and accreditation. Surgical team beyond the lead surgeon (anesthesiologist, OR nursing). Responsible safety data where available, with enough context to avoid misleading patients. Facility certifications. The patient is flying to a country where she does not know the regulatory landscape. Your safety section is where you make that landscape legible.
Pricing and package context
A starting price range with what is included and what is not. Hospital stay, surgeon fees, anesthesia, post-op medications, follow-up calls, nutritional consultation, lab work, transportation, hotel. Be explicit about what is in the package and what costs extra. Pricing pages are the single highest-leverage piece of content for AI extraction in bariatric. Hiding the number behind a form just means the AI assistant pulls a number from your competitor. The longer argument is in our AI pricing transparency for Tijuana medical tourism breakdown.
Travel and stay timeline
A day-by-day timeline from arrival to departure. Day 1: arrival, labs, consultation. Day 2: surgery. Day 3 to 4: recovery in hospital. Day 5: discharge, hotel rest. Day 6 to 7: follow-up, return home. This section answers a question that is high friction for cross-border patients and almost never addressed on clinic sites with the specificity it deserves.
Recovery timeline
What recovery actually looks like. Liquid diet phase, soft food phase, full food reintroduction. Energy levels week by week. Return to work expectations. Physical activity progression. Patients comparing clinics often pick the one with the most concrete recovery timeline. Vagueness loses to specificity here.
Aftercare and returning home
The cross-border patient's biggest unanswered question is what happens if something goes wrong after she gets back to the US. Post-op communication plan, scheduled follow-up calls, partner network in the US, emergency protocol, nutritional support, labs to do at home, vitamin supplementation requirements. This section is the last objection killer. It is also the most underdone section on most Tijuana bariatric pages.
Reviews and patient proof
Specific reviews. Procedure named, surgeon named, recovery timeline mentioned, outcome described. A wall of five-star reviews that say "great experience" is noise. One detailed four-star review can be more useful than a wall of generic five-stars. The unfortunate truth is that most clinics let their best reviews stay generic because nobody trains the coordinator to ask the patient to be specific. Fix that. The how, including ethical review prompting, is in our bariatric surgeon reviews guide.
FAQ section
Each question answered directly in 40 to 60 words, then expanded if needed. This is the most extractable content type for AI assistants and Google AI Overviews. Use the patient question list from earlier in this article as your source. Do not waste FAQ space on questions no patient is actually asking.
CTA to consultation or scorecard
End with a single, clear next step. Not three CTAs competing for attention. Not a chat widget that fires after 8 seconds. One direct action: book a consultation, request a quote, or take the next research step the patient is actually ready for at that point in the page.
Internal links
From this gastric sleeve page, link to the surgeon page or pages, the pricing page, the safety page, the bypass comparison page, the reviews page, and the broader bariatric SEO guide where relevant. From those pages, link back to this one. This is the linking pattern that helps Google understand the relationship between procedure, surgeon, and outcome, and helps AI systems retrieve consistent answers across the practice.
How AI systems read a gastric sleeve page
AI does not match keywords the way Google did in 2015. It summarizes what it can retrieve and verify. The shift from match to summary is the entire reason this article exists.
For a gastric sleeve page, that means AI systems need extractable, consistent, internally connected evidence on procedure, surgeon, location, candidate profile, package, pricing, safety, recovery, aftercare, and proof. Each one is a node. The page either supplies the node clearly or it does not.
AI cannot confidently explain what it cannot clearly extract.
When the extraction is strong, AI has more material to retrieve, compare, and explain when a patient asks a question that touches your practice. When the extraction is weak, AI has less to work with, and a competitor with cleaner evidence gets cited in the patient's answer.
This is not about AI recommending your clinic. No one can promise that. It is about whether the patient who asked an AI assistant for the best gastric sleeve surgeon in Tijuana sees your name in the answer at all. If you are absent from the answer, you may be absent from the patient's consideration set, regardless of where your page ranks in traditional search.
The deeper version of this argument is in AI visibility for Tijuana surgeons.
AI Extraction Simulator: Thin page vs decision-support page
AI cannot confidently explain what it cannot clearly extract. Pick a patient question and compare what a generic gastric sleeve page gives AI versus what a decision-support page makes extractable.
Interactive demo: toggle between a thin page and a decision-support page, then pick a patient question to see how much an AI assistant can extract and how confident its answer is. The short version: a thin page leaves AI guessing on pricing, surgeon, candidacy, safety, and aftercare; a decision-support page makes every one of those extractable.
Gastric sleeve SEO checklist
A practical checklist. If you can answer yes to each, your gastric sleeve page is doing modern work.
- Page indexed and crawlable, with a clean URL and no duplicate content issues.
- Clear, descriptive H1 that includes the procedure and a value differentiation when appropriate.
- Short direct answer in the first 150 words of body content.
- Surgeon or surgeons connected by name, linked to dedicated surgeon pages.
- Procedure technical details with appropriate medical accuracy.
- Candidacy and BMI section with concrete thresholds.
- Pricing context with starting range and package inclusions.
- Hospital and facility safety information.
- Day-by-day travel and stay timeline.
- Recovery timeline with concrete week-by-week markers.
- Aftercare protocol for patients returning home to the US.
- Specific reviews mentioning procedure, surgeon, and outcome.
- Internal links to surgeon, pricing, safety, reviews, and bypass comparison.
- FAQ block answering real patient questions in extractable format.
- Schema markup for the procedure and the connected surgeon, where accurate.
- Prompt tracking baseline established for "gastric sleeve Tijuana" and related queries. See how to build a prompt tracking baseline.
- Conversion tracking that goes beyond the form submission to consultation booked and surgery booked.
- Self-reported attribution captured at the consultation stage.
Most practices have items 1 through 5. The work that compounds is items 6 through 18.
How this connects to the bariatric SEO guide
This article is the procedure-page deep dive that the broader guide argues for. Our guide, SEO for bariatric surgeons, explains the whole system: the patient decision journey, the failure modes of old bariatric SEO, the AI visibility layer, the prompt-mapping logic, and the modern checklist.
This piece zooms into the single most important page type in that system: the gastric sleeve procedure page. A practice cannot win modern bariatric SEO with generic procedure pages, no matter how many backlinks point at them or how well-tuned the title tags are. The procedure page must become a decision-support asset for both the patient and the AI systems that summarize it.
A worked example of this approach applied to a multi-surgeon bariatric practice is in our VIDA case study.
Start with the Scorecard
If you want to know whether AI can already find, name, and explain your gastric sleeve practice, start with the Free AI Visibility Scorecard. It will tell you whether your surgeons are findable, whether your gastric sleeve page is extractable, where external sources support your claims, and where the gaps are.
It will not promise that AI will surface your clinic tomorrow. No one can promise that. What it will tell you is whether the evidence layer your gastric sleeve practice depends on is intact or missing.
Quick answers
What is gastric sleeve SEO?
Gastric sleeve SEO is the discipline of structuring procedure pages, surgeon connections, pricing context, and external corroboration so that gastric sleeve content is findable in traditional search, extractable by AI assistants, and useful to patients comparing clinics before any form is filled.
What should a gastric sleeve procedure page include?
A direct answer, candidacy criteria with BMI thresholds, named surgeons, procedure details, sleeve vs bypass comparison, safety and facility information, transparent pricing context, travel and stay timeline, recovery timeline, aftercare for US patients, specific reviews, internal links to related pages, FAQ block, and a clear single CTA.
Why is pricing context important for gastric sleeve SEO?
Patients comparing cross-border gastric sleeve are price-aware by definition. If your page does not publish a starting range with package context, AI assistants may rely on competitor sites or other public sources instead. You either control the narrative or someone else does.
How does AI visibility change gastric sleeve marketing?
AI assistants summarize what they can retrieve and verify. Practices with extractable, internally consistent, externally corroborated evidence give AI systems more usable material to work with. That can help patients reach the consultation with more trust already built.
Should every bariatric surgeon have a separate gastric sleeve page?
The practice should have a gastric sleeve page that names the specific surgeons who perform it, with links to each surgeon's dedicated bio. If only one surgeon in the practice performs sleeve, the page should still surface that surgeon clearly rather than hide behind "our team of experienced surgeons."
How does this connect to SEO for bariatric surgeons?
The bariatric SEO guide explains the full system: patient journey, AI visibility layer, measurement gaps, and content strategy. This article is the procedure-page deep dive that guide argues for. Together they describe how a modern bariatric practice structures content for both search engines and AI assistants.